Evaluation and Treatment of Hypothermia, Colin K. Grissom, M.D.
page 5
effort is initially stimulated during mild hypothermia because of increased carbon dioxide
(CO
2
) production from shivering, continued drop in core temperature results in decreased
VO
2
and respiratory rate slows. Oxygen consumption (VO
2
) and CO
2
production are 50%
of normal at 28°C. Cessation of shivering results in a state of poikilothermia where core
body temperature will eventually equilibrate with environmental temperature. Reduction
in cerebral metabolism causes a decline in cerebral blood flow of approximately 6% for
every °C fall in core temperature. At temperatures near 30°C confusion, ataxia, and
dysarthria appear. Hypothermic depression of enzymatic processes occurring within the
kidney leads to sodium and glucose losses in urine. Since electrolyte and glucose losses
promote osmotic diuresis, hypovolemia and dehydration may occur.
Clinical Presentation: Severe Hypothermia
With continued cooling to temperatures resulting in the severe hypothermia range
(below 28°C) ventricular fibrillation (VF) may occur. Patient manipulations during
transfers or chest compressions for bradycardia or hypotension may precipitate VF or
asystole. EKG changes include prolongation of PR, QRS, and QT intervals, nonspecific
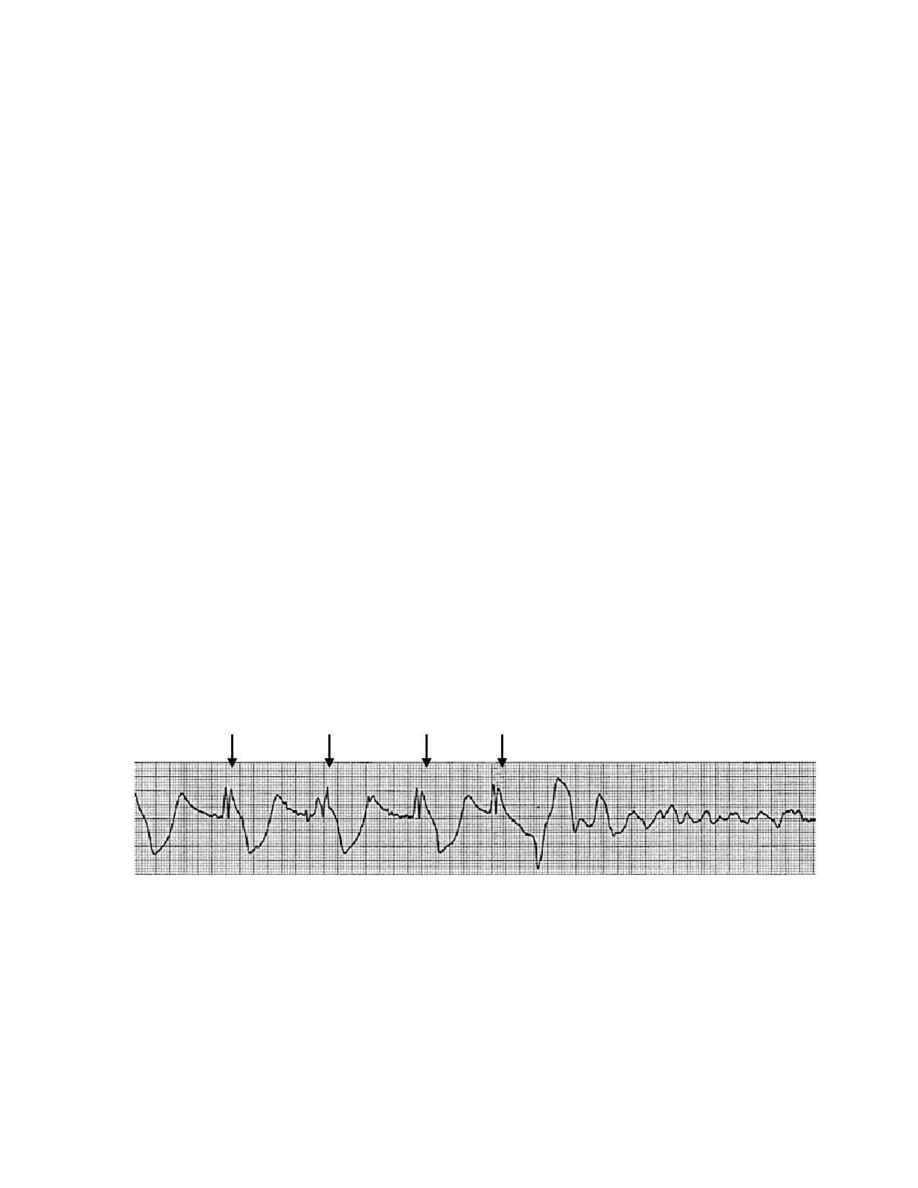
ST and T wave changes. Osborn waves (or "J" waves) seen on the EKG are usually
pathognomonic of hypothermia (Figure 1), but are present less than 50% of the time.
In severe hypothermia mental status is severely depressed resulting in stupor or
coma. Coma occurs at temperatures nearing 25°C. Pupillary reflexes and deep tendon
reflexes are diminished or absent. Respiratory effort may be undetectable. With cooling
to temperatures below 25°C, circulatory arrest may result from VF or asystole.
Until cardiac arrest occurs, it should be remembered that despite the clinical
appearance, hypothermia is protective. Suppression of enzymatic energy dependent
processes markedly diminishes oxygen and metabolic demands. These decreased
requirements explain the successful resuscitation of some hypothermic victims despite
the appearance of death.
Figure 1. Osborn J waves (arrows) after the QRS followed by ventricular
fibrillation secondary to jostling during an ambulance ride in a hypothermic patient
(Danzl 2002).