Wilderness Medical Society snowmass 2005 Page 110
Colin Grissom, M.D. "New Hope For Surviving the Avalanche"
Page
4
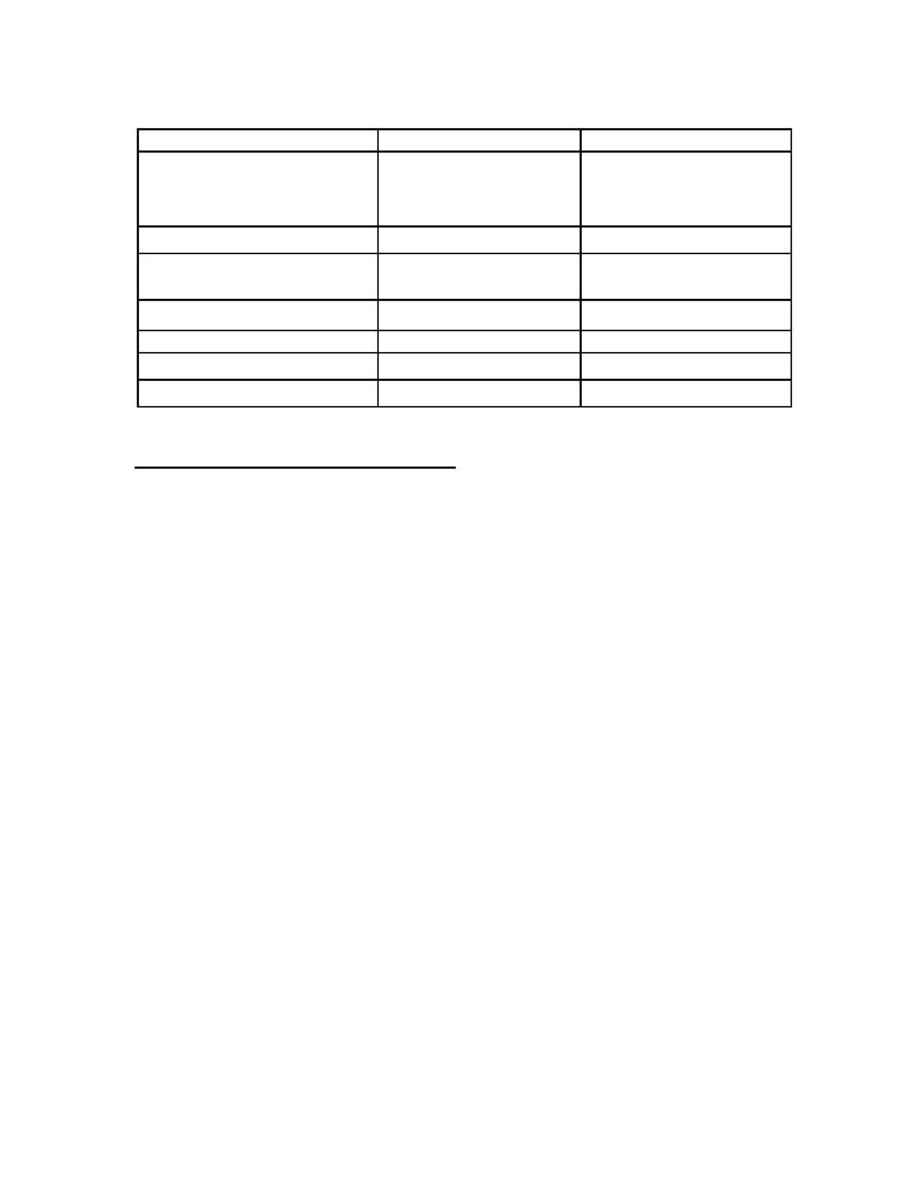
Table 2. Injuries in Survivors of Avalanche Accidents (partial and total burials)
13
Utah Europe
Total Injuries
9
(total 91 avalanche
accidents)
351
(total 1,447 avalanche
accidents)
Major Orthopedic
3 (33%)
95 (27%)
Hypothermia requiring
treatment at hospital arrival
2 (22%)
74 (21%)
Skin/Soft Tissue
1 (11%)
84 (25%)
Craniofacial
83
(24%)
Chest
3 (33%)
7 (2%)
Abdominal
4
(1%)
Respiratory Physiology of Avalanche Burial
Asphyxiation occurs during avalanche burial because the victim inhales snow
occluding the upper airway or because expired air is re-breathed. Acute upper airway
obstruction resulting in asphyxiation is one of the causes of early asphyxiation during the
first 15 to 30 minutes of avalanche burial. Asphyxiation due to re-breathing expired air
may also occur during the first 15 to 30 minutes of avalanche burial if there is no air
pocket for breathing, or may be delayed if an air pocket is present. Inspired air contains
21% oxygen (O2) and less than 0.03% carbon dioxide (CO2), while expired air contains
about 16% O2 and 5% CO2. Rebreathing expired air in an enclosed space results in
progressive hypoxia and hypercapnia that will eventually result in death from
asphyxiation. The larger the air pocket the greater the surface area for diffusion of
expired air into the snowpack and diffusion of ambient air from the snowpack into the air
pocket, and the longer the survival time before death occurs from asphyxiation. Ice mask
formation around the avalanche victim's face will accelerate asphyxiation by preventing
diffusion of expired air away from the air pocket in front of the mouth. Ice mask
formation occurs when water in heated and humidified expired air freezes on the snow
surface in front of the face forming a barrier that is impermeable to diffusion of air.
The physiology of asphyxiation from breathing with an air pocket in the snow
was demonstrated in a study by Brugger and colleagues
8
where subjects breathed into one
or two liter volume air pockets in snow of similar density to avalanche debris (density
150 to 600 kg/m3 or 15 to 60 % water). Subjects sat outside a snow mound and breathed
through an air-tight mask connected by respiratory tubing to a one or two liter volume air
pocket in snow. The initial fraction of inspired oxygen (FIO2) in the air pocket was 21%,
and the initial fraction of inspired carbon dioxide (FICO2) was near 0%. As expired air
was rebreathed in the air pocket, FIO2 decreased to about 10% and FICO2 increased to
about 6% over 30 minutes (Figure 2). These changes in O2 and CO2 in the air pocket
resulted in a decreased arterial O2 saturation as measured by a pulse oximeter (SpO2 %)
and an increased end tidal CO2 (ETCO2) partial pressure. Most subjects were not able to
complete the entire 30 minutes of the study and had to stop secondary to dyspnea,
hypercapnia, and hypoxia. This study demonstrates the respiratory physiology of