SSMC Employee Health Benefit Plan
8
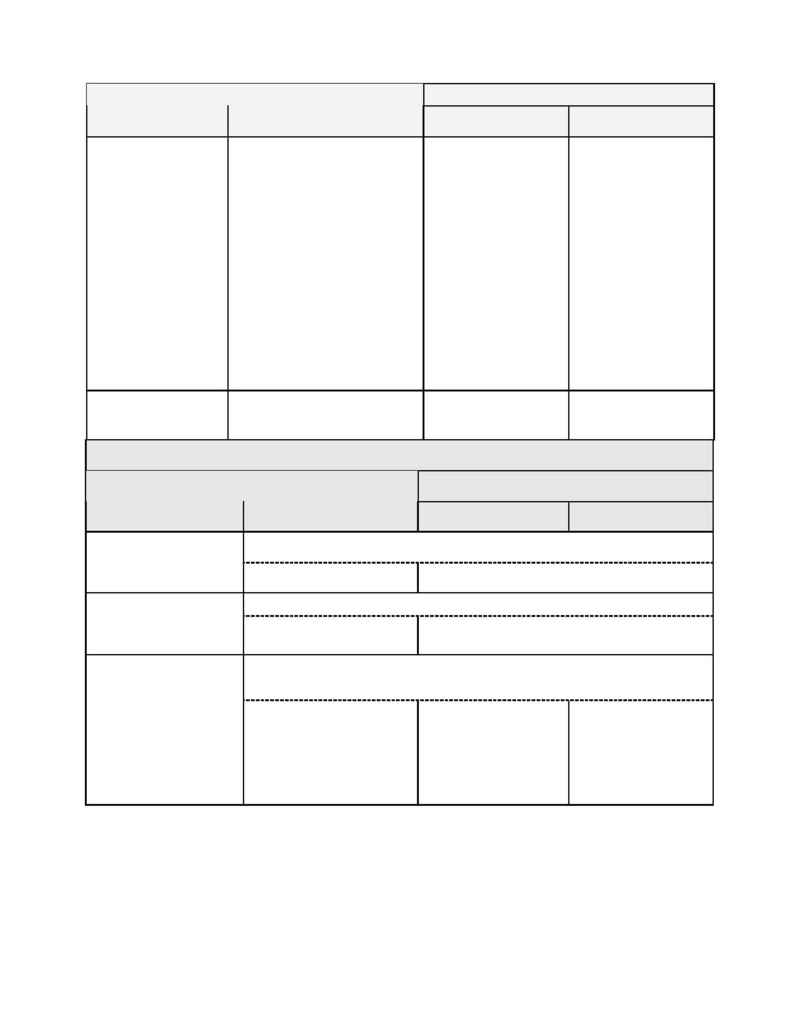
Out-of-Network Providers
Schedule A
Deductibles and
Copayments
PHO Area Network Providers
Living In PHO Area
Living Out of PHO Area
Out-of-Pocket
Deductible and
Copayment
Maximum.
Does not Apply
Does Not Apply
The most you will have
to pay for any
combination of
Deductible and 20%
Percentage Copayment
is:
Individual: $600 per
Calendar Year.
Family:
$800 per
Calendar Year
After these Out-of-
Pocket maximu ms have
been exceeded, the Plan
pays 100% of most
Allowable Fees for the
remainder of the
Calendar Year.
PHO Network
Copayment
$5.00 per visit
Does not apply
Does Not Apply
Schedule A Preventive Care Expenses
Out-of-Network Providers
Schedule A
Preventive Care Expenses
SSMC
PHO Area Network
Providers
Living in PHO Area
Living Outside PHO Area
Frequency based on age and medical history
Routine Mammography
Plan pays 100%
No Deductible. Plan pays 100%
Coverage limited to once per Calendar Year for Covered Females, age 18 or older.
Routine Pap Test
Pap Test. Plan pays 100%
Related Exam: Not Covered.
Pap Test. No Deductible. Plan pays 100%
Related Exam. Not Covered.
Frequency based on age. Coverage includes routine nursery visits, well-child exams,
immunizations and related tests.
Well Child Care
Screening Tests and
Immunizations:
Plan pays 100%.
Nursery exams and Office
Visits:
$5.00 Network
Copayment per visit.
Screening Tests: No
Deductible. Plan pays
100%.
Other Routine Child
Care: After Deductible
pays 70%
Screening Tests: No
Deductible. Plan pays
100%.
Other Routine Child
Care: After Deductible
pays 70%